CAPÍTULO 21 TEAR FILM DEFICIENCY IN DRY EYE DISEASE: Gysbert B. van Setten |
| THE TEAR FILM IN DRY EYE
DISEASE In dry eye disease clinical symptoms vary from itching and red eyes to most intense irritation, scarring, corneal neovascularization and formation of symblepharon. In the most severe cases the final stages include the transformation and cicatrization of conjunctival epithelium. Also the conjunctival epithelial damage shows a high correlation with corneal epithelial damage stained with fluorescein (Suzuki et al 1997). In the pathophysiology a great variety of factors are involved and there is increased awareness that dry eye disease is much more than just a deficit of tear fluid. Other factors such as evaporation rate, lid positioning, meibomian gland function play a major role and have been reviewed (Rivas et al. 1992, Pérez-Domingo et al. 1996). All these factors seem related in a rather complicated interaction and more or less complex models have been created. Pflugfelder suggested recently a practical classification of dry eye disease into those with adequate aqueous tear production and those with aqueous tear deficiency. Aqueous tear deficiencies leading to a family of ocular surface disease, termed keratoconjunctivitis sicca (KCS) may be further subclassified into non-Sjögren's syndrome and Sjogren's syndrome (SS) groups. (Pflugfelder 1996). Aqueous tear film deficiencies involve a deprivation of the ocular surface from a variety of different agents. One small group of agents with nevertheless major physiological importance is the group of growth factors. By today a considerable number of growth factors have been detected in tear fluid (table 1).
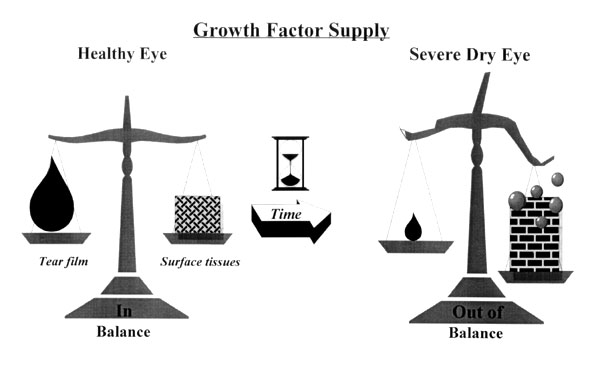
ORIGIN OF GROWTH FACTORS IN TEARS The lacrimal glands and the ocular surface Many of the growth factors present in the aqueous phase of the tear film is derived from the lacrimal gland tissue. This has been shown for EGF (van Setten et al. 1990), TGF- a (van Setten et al. 1996). A significant role of these growth factors for corneal physiology has been suggested. According to current models the decrease of aqueous tear production should result in a decreased growth factor concentration in their tears (van Setten et al. 1992). The most common decrease of tear fluid secretion is known to occur with age (De Roetth 1952). However, only a certain percentage of elderly patients experience dry eye symptoms and pathology. Also is there, to the best knowledge of the author, no study yet convincingly showing low levels of tear fluid derived growth factors in the tear fluid of the elderly, even if a slight decrease of tear fluid secretion might be measurable. Also, that far a significant decrease of growth factor concentration has not been shown in the tears of dry eye patients. Naturally this might be due to the difficulties of collecting sufficient amounts of tears from dry eye patients. On the other hand also an increased supply by ocular surface tissue itself must be considered. Human corneal epithelium contains for example EGF, TGF a (Khaw et al.1992), bFGF (van Setten 1996) and VEGF (van Setten 1997) as well. As dry eye disease often is associated with epithelial disorders of varying intensity. Loss of defective epithelial tissue is in turn calls for compensation, causing the surrounding tissue to enhance proliferation. With a the resulting augmented turn over rate of epithelial cells an enhanced production and release of growth factors to the remaining tear film layer might occur. Autocrine and paracrine mechanims were suggested. Upregulation of growth factor release would lead to an imbalance in the growth factor system in dry eye disease. This could be one major responsible factor for the increase of more squamous metaplasia in patients with Sjögren syndrome (Takamura et al. 1994, Tsubota et al. 1994).
Other sources of growth factors and their release mechanisms: the role of the leucocytes This imbalance of growth factor secretion from ocular glandular tissues and the ocular surface could be significantly enhanced by a third, still most neglected factor, the inflammation associated with dry eye disease. Both chronic blepharitis due to infections and toxic blepharitis due to excessive treatment are known to occur in dry eye disease (Heiligenhaus et al. 1994). Also are chronic inflammatory diseases of the conjunctiva itself considered to lead to the socalled dry eye syndrome (Marquardt 1990). Of course does chronic inflammation also alter the tear film due to changes at the ocular surface. Conjunctival goblet cell density, for example, decreased and epithelial stratification increased as the degree of submucosal inflammatory cell infiltration increased (Johnson et al. 1990). Inflammation is associated with the release of leucocytes to the ocular surface. Also minor ocular surface damage in dry eye leads to leucocyte evasion into tear film similarly as it has been shown for ocular surface damage. Activated leucocytes in turn are known to harbour a great variety of growth factors, some of which have not been shown to occur normaly in tear film. It is known that polymorphonuclear leukocytes (PMNs) emerge first in local inflammatory sites. Some of the mediators released by PMNs, such as transforming growth factor-beta1 (TGF b 1), additionally trigger the accumulation of further leucocytes stimulating extravasal emigration (Drake & Issekutz 1993) and chemotaxis (Balazovich et al. 1996). The evasion of PMNs is followed by macrophages. Macrophages are phagocytic cells accumulating at the sites of tissue lesion. Involved in the remodelling of tissues, they are loaded with various cytokines, amongst them various stimulators of wound healing such as bFGF, TGF- a , PDGF, HB-EGF and various ILs. Two of the many factors present in leucocytes, that is IL-1 and TNF appear to play a major role in coordinating the inflammatory mechanism (Cavaillon & Haeffner-Cavaillon 1993). Recent studies thus suggest that inflammatory processes may be positively and negatively controlled by a quantitative factor of initial PMN populations by regulating the TNF release activity of the subsequent macrophages (Yui et al. 1993). The regulation of macrophage activation is, due to the interaction with various factors, very complex (Bogdan et al. 1993). Reviews about the various growth factors in these cells have been given in large number and literature around this subject is increasing rapidly. Considering dry eye and associated diseases there is increasing evidence the transition from inflammation to scar tissue may be triggered by the immuno-mediated secretion of fibrogenic cytokines in various fibrosing conjunctival disorders (Bernauer et al. 1993). One possible example is acute ocular cicatricial pemphigoid where, the conjunctiva is infiltrated with, amongst others neutrophils and macrophages (Elder & Lightman 1994). The increased presence of leucocytes at the ocular surface necessarily also leads to enhanced presence of their growth factors in the remaining tear film. It is, however, unknown how long such factors remains detectable in tears as some of the released cytokines such as TNF- b bind to extracellular matrix proteins, i.e. laminin and fibronectin (Hershkoviz et al. 1995). Interestingly enough it is just these proteins that are deposited at the surface of injured tissues. A possible role of bacterial infections causing imbalances of the growth factors at the ocular surface might be suggested. Interestingly enough, however, it seems to be the inflammatory processes themselves and not an increased incidence of bacterial infections that alters the growth factor balance at the ocular surface, although it has been shown that together with a decrease of the secretion of aqueous tears also the availability of antibacterial substances decreases (Seal et al. 1986). However, it is not only the release of growth factors themselves due to degranulation processes that alters the sensitive balance of cytokines at the ocular surface in eyes with chronic inflammation. The enzymatic liberation of growth factors stored in the tissue forming the ocular surface due to enzymes secreted by activated inflammatory cells may significantly contribute to increased local presence of growth factors in both media, i.e. tear fluid and tissues. Basic FGF, for example, found to exist in corneal epithelium (van Setten 1996) is bound to heparan sulfate (HS) in the ECM (extracellular matrix) and is released in an active form when the ECMHS is degraded by heparanase expressed by cells such as platelets, neutrophils (Vlodavsky et al. 1991). Metalloproteinases, released by macrophages may have similar effects. This was recently shown for TNF- a (Goetzl et al. 1996). Clinically of major importance is also the fibrinolytic system of the tear film which has been ealier shown to be activated in ocular surface disease (van Setten 1991). Accordingly only recently the macrophage stimulated urokinase-type plasminogen activator (uPA) associated increased release of matrix-bound bFGF was demonstrated (Falcone et al 1993). In summary, there are three major pathways leading to the deliberation of growth factors at the surface of the dry eye and its tear film, causing a change of balance in this very sensitive system of very powerful agents. The inflammatory response in the ocular surface tissues may constitute a major reservoir of growth factors altering the clinical picture and accessibility of severe dry eye disease. Its increased understanding could considerably contribute to a more effective therapy of dry eye disease. The effects of cytokines on tissues does however, depend to a major extent upon the presence and functionality of the specific receptors. This, in turn, is a highly unexplored and complex area and will be adressed to elsewhere.
Acknowledgements The author is very thankful to the Karolinska Institute's committee for FOUU, Stockholm, Sweden for the generous support. |