REQUESTED PUBLICATION
Pigmentary dispersion syndrome after phakoemulsification and intraocular lens implant
MÉNDEZ HERNÁNDEZ C1, MUÑOZ AM2
San Carlos Clinical Hospital. Complutense
University, Madrid.
1 Glaucoma Dept.
2 MIR.
ABSTRACT
In recent years pigment dispersion cases have been described after the implant of single block intraocular lenses (IOL) in sulcus after cataract surgery, without or without posterior capsule tear. The mechanisms which give rise to pigment dispersion are, among others, increased contact between the iris and the lens, as well as a tendency to a certain degree of mobility of the IOL in the posterior chamber, which appear to be more associated to some IOL designs.
This paper presents a 7-case series of pigment dispersion in pseudophakic patients after the implant of a single piece IOL in sulcus and/or capsular sac, including a revision of this conditions, the possible predisposing factors and those which could help in a diagnostic as well as therapeutic options.
Key words: Pigment glaucoma, pigment dispersion syndrome, iridotomy, ultrasound biomicroscopy, cataract surgery, intraocular lens.
INTRODUCTION
Pigmentary glaucoma (PG) is one of the most frequent forms of open angle secondary glaucoma. It is a consequence of an obstruction in the aqueous humor flow at the level of the trabecular mesh, secondary to the dispersion of iridian pigment in the anterior chamber. This dispersion of pigment accounts for the typical clinical findings of the pigment dispersion syndrome (PDS) and PG such as the Krukenberg spindle, transillumination in the mean periphery of the iris, trabecular mesh hyperpigmentation and pigment deposits in the zonule, anterior surface of the iris and lens, although sometimes the typical iridian transillumination defects may not be evident in very dark-colored iris (1). PG and/or PDS, secondary to an intra-ocular lens (IOL) implant after cataract surgery could arise due to excessive manipulation during the intervention or also in the post-op. In the latter case, the main pigment dispersion mechanisms are contact between the iris and lens and the presence of IOL mobility in the posterior chamber due to instability. As with phakic lens posterior chamber implants, the pigment dispersion is more frequent when the implant is in the sulcus due to the smaller distance between the IOL and the iris pigmentary epithelium (2-7). Other factors include the inadequate size of the lens vis-à-vis the sulcus-sulcus distance and its design and materials (8-11). Pigment dispersion has also been described in IOL capsular sac implants after cataract surgery without complications. Placing in the sulcus at least one of the IOL haptics was the cause of the pigment dispersion in the majority of cases, although pigment dispersion has also been described in pseudophakic patients having both haptics implanted in the capsular sac (12-18).
We present a series of 7 pigment dispersion cases in pseudophakic patients after implant of an AcrySof SN60AT (ALCON, Inc) IOL in sulcus and/or capsular sac, diagnosed at the Glaucoma Dept. of our Hospital.
RESULTS
Table 1 shows the age and sex of patients, the date of the cataract surgery and the time elapsed before the pigment dispersion appeared. The findings at diagnostic time are shown in Table 2.
All the patients were intervened for cataracts with phakoemulsification between 2004 and 2007, and all were implanted AcrySof SN60AT lenses. In 4 of the 7 patients, the IOL was implanted in sulcus due to posterior capsule tear during the surgery, and in the 3 remaining cases it was made in the capsular sac and the surgery proceeded without complications. In 2 of said 3 patients, the cause of pigment dispersion was identified as the displacement to the sulcus of one of the haptics by means of anterior chamber ultrasound biomicroscopy (UBM). In one case both haptics were in the capsular sac, although one had shifted to a more anterior plane, causing the pigment dispersion.
In the majority of cases (5 out of 7 patients), over a year elapsed from the implant date until they were referred to our Dept. for assessment.
At diagnostic time, the mean IOP was of 15.57 mmHg and all patients exhibited pigment dispersion and iridian transillumination. None of the lenses was dislocated and all the patients had good uncorrected visual acuity (UVA), between 20/20 and 20/40. Two patients exhibited repetition uveitis which improved with topical corticoid and hypotensor treatment. No additional complications were detected in relation to cataract surgery or IOL implant.
Table 3 shows the treatment, the IOP and final UVA.
In all the patients good IOP control was achieved with selective laser trabeculoplasty (SLT) and medical treatment. In 3 patients SLT was performed with good results. In one case the IOL was explanted and replaced by a 3-piece IOL in sulcus due to hypertensive uveitis and blurred vision with insufficient response to frequent inflammation episodes which failed to respond to medical treatment. After replacing the IOL, the uveitis events remitted and IOP remains within normal limits without medical treatment, with UVA being of 20/40.
Three of the 7 cases of said series are described below.
Case 1
A 77-year old emmetrope female without relevant ocular history, with a corrected visual acuity (CVA) of 20/100 in the right eye (-1.75-0.50x29º), intervened for cataracts (phakoemulsification without complications, 5 mm capsulorhexis) with 20D AcrySof SN60AT implant. Two weeks after the intervention, pigmented tyndall was evidenced in anterior chamber and over the IOL together with sectoral iridian transillumination (fig. 1). Her UVA was of 20/32 and IOP without treatment of 15 mmHg.

Fig. 1. Iridian transillumination in a patient with AcrySof IOL implant in
sulcus.
An UBM revealed an IOL implant with both haptics in the capsular sac. One of the haptics had shifted to a more anterior plane, making contact with the anterior capsule and touching the iris posterior epithelium.
During follow-up, the IOP remained within normal limits without hypotensor treatment. Figures 2a and 2b illustrate the capsulorhexis limit and the IOL implant in the capsular sac. Figure 3 shows the imprint of the haptic on the iris.
![]()
Fig. 2. Anterior chamber UBM, showing the capsulorhexis limit (arrows) and the
IOL implant in capsular sac. Courtesy of Professor García Feijoó.
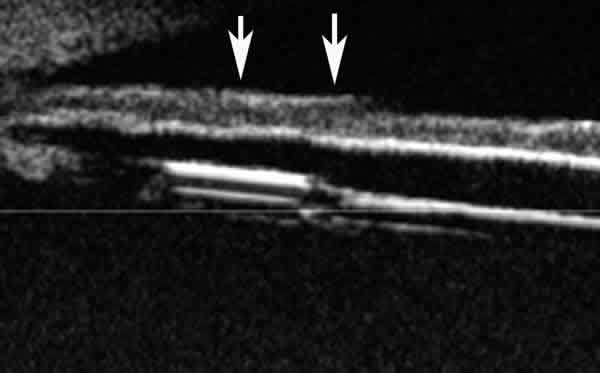
Fig. 3. UBM image showing the imprint of the inferior IOL haptic in the
pigmentary epithelium of the iris (arrows). Courtesy of Professor García Feijoó.
Case 2
A 65-year old female with ocular hypertension history in treatment with a drug, CVA of 20/100 in right eye (+3.00-1.25x88º) intervened for cataracts via phakoemulsification without complications and 26 D AcrySof SN60AT IOL implant in capsular sac. The post-op was free of events (UVA 20/32). A routine ophthalmological assessment made one year after surgery revealed iridian transillumination following the path of the inferior haptic and pigment on the IOL (figs. 4 and 5) and IOP 17 mmHg without medical treatment. The anterior chamber UBM evidenced a displacement of the capsular sac inferior haptic to the sulcus. Three years after surgery, the untreated IOP increased to 25 mmHg. Gonioscopy showed anterior synechiae in approximately the lower 180º (fig. 6). Medical treatment was established and subsequently an SLT was performed (1 session, inferior 1/2, 58 impacts, 0.7 mJ). Five years after the intervention, the IOP is at 18 mmHg with two drugs, campimetry is normal (Perimetry TOP G1, DM 0.9 dB, LV 3.8 dB) and UVA of 20/32.

Fig. 4. Iridian transillumination following the IOL haptic path.
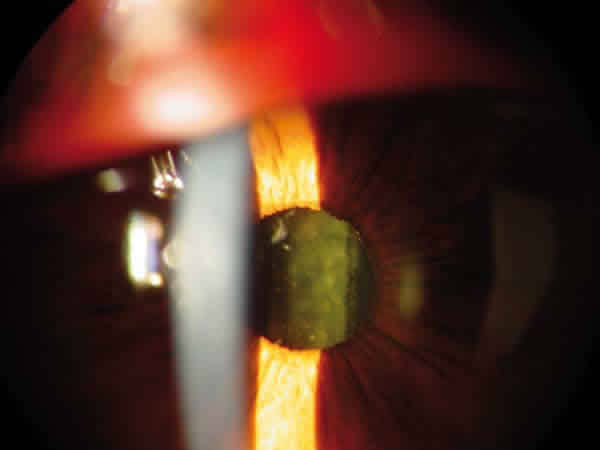
Fig. 5. Pigment on IOL in a patient with pigment dispersion after AcrySof
IOL implant in sulcus.

Fig. 6. Angle showing a marked pigmentation increase.
Case 3
A 64-year old emmetrope male without ocular history, with a CVA of <20/200 in the RE (-4-1.75 x167º) operated for cataracts with phakoemulsification. During the IOL implant in sac (20 D AcrySof SN60AT), a posterior capsule tear occurred, for which reason the surgeon decided to place it in the sulcus. The post-op did not exhibit IOL increase, pigment dispersion or other complications. The patient’s UVA was of 20/40. Five years after the operation, the patient was referred for assessment to our department due to an IOP of 42 mmHg in RE. The UVA was of 20/40 and the exploration revealed pigment in the iris and iridian transillumination in the superior nasal quadrant. Gonioscopy evidenced a pigmented grade IV angle and anterior synechiae in less than one quadrant. The TOP G1 visual field exhibited a superior arch-shaped scotoma (DM: 2.5 dB, LV: 12.8 dB). The papillary rim was of 0.3 in RE and 0.1 in LE. An SLT was performed (one session, lower half, 50 impacts, 0.6 mJ) maintaining good tension control with two drugs 4 months later.
DISCUSSION
In all the cases of this series the lens implanted in the capsular as well as in the sulcus was AcrySof SN60AT.
As occurred with some cases described by Chang et al (21), in the majority of patients of our series the pigment dispersion was first described years after the surgery. All had good uncorrected far visual acuity and good IOP control was achieved with medical treatment or laser trabeculoplasty. One of the patients exhibited episodes of hypertense uveitis and blurred vision which did not respond to the medical treatment. For this reason it was decided to replace the single block lens by a 3-piece IOL in sulcus. After the replacement, the uveitis events remitted and the IOP remained within normal limits without medical treatment, although the UVA was from 20/20 to 20/40.
In the rest of cases the IOP remained within normal limits without detecting progression. For this reason it was decided to adopt a conservative approach considering the UVA, the time elapsed since the surgery and the good IOP control.
The implant of a single block lens in sulcus involves higher risk of complications, including PDS and PG. The pigment dispersion in pseudophakic with IOL implant in capsular sac or sulcus seems to be more frequent or accentuated with some IOL models such as AcrySof SN60AT (15,16,18-20). Several factors could assist in this fact. The square edge of the optic zone and haptics, the design which could contribute to a greater contact surface between the IOL and iris and the flexibility of the haptics which facilitate its movement in the antero-posterior axis, with a tendency to adopting concave position with the ends of the haptics displaced forward, locating in a more anterior plane than the rest of the IOL. Although the SPD or PG is more frequent in cases where the AcrySof lens is implanted in sulcus (19,20), it has also been described in cases of sac implant where the lens displaced anteriorly due to an excessively broad capsulorhexis or de-centering of the IOL which could facilitate one of the haptics or a part of the optic zone taking a more anterior position (15,16,18). A haptic located in front of the capsulorhexis could give rise to iris indentation, pigment dispersion and sectorial pigmentary epithelium atrophy.
For the same reason, the pigment dispersion would also be more frequent after performing the piggyback technique (6,7).
In case of posterior capsule tear, an IOL implant having a
degree of instability in the sulcus will exhibit a greater tendency to disperse
pigment as it changes position. A single block IOL or with a relatively large
diameter vis-à-vis the sulcus-sulcus distance, with flat morphology, small angle
in the junction between the optic zone and the haptics, will have some degree of
anterior mobility and more de-centering risk if implanted in sulcus. If the IOL
has a tendency to anterior displacement of some of the haptics, the probability
of pigment dispersion will be greater. PDS secondary to IOL generally produces
clinical symptoms in the first post-op months or weeks. The anterior chamber
pigment associated or not to increased IOP could be mistaken in some cases with
an increase of post-op inflammation. Hyper-pigmentation in the angle and local
iridian transillumination areas, sometime associated to an imprint of the
haptics responsible for the friction with the pigmentary epithelium can assist
in the differential diagnostic.
Anterior chamber exploration techniques such as OCT or UBM (15,17,18) allow an
analysis of the anatomic relationships of intraocular lenses and also to locate
the intra-extrasacular situation of the optic zone and haptics.
If the pigment dispersion is accompanied by increased IOP, an expectant attitude can be maintained, controlling IOP with medical treatment or laser trabeculoplasty, opting for lens explant in the cases where the IOP could not be controlled, as a chronic pigment dispersion could lead to an irreversible damage of the trabecular mesh. As we know, trabecular mesh damage in long evolution cases could be irreversible due to the pigment overload.
In a broad revision of complications after implant of single block acrylic IOL in sulcus made by Chang et al (21), 83.3% of patients (25 out of 30 cases) exhibited pigment dispersion and, even though the authors did not relate the complications identified in the series with the type of implanted lens, in 20 of the 30 cases the implanted lens was AcrySof SA60 AT. Of the 10 remaining patients, 9 had an IOL with a similar morphology: 6 AcrySof SN60 WF IOL, 1 Restor IOL, 1 thoric ALCON IOL and AcrySof IOL of unknown model (table 4). Most of the IOLs implanted in this series shared the same characteristics: a short total length for being implanted in sulcus without risk of dislocation and anterior and posterior surfaces with thick and marked square edges both in the optic zone as in the haptics and flexible haptics. This morphology could partly explain the cases of pigment dispersion described in the literature, even in spite of a capsular sac implant.
Chang et al recommended to abstain from implanting single block acrylic lenses in sulcus due to the risk of complications such as pigment dispersion. On the other hand, some precautions should be taken when implanting said type of lenses in capsular sac, such as not implanting them in case of very wide capsulorhexis, making sure that both haptics have opened completely in the capsular sac, checking their proper location before closing the intervention and that the capsulorhexis should cover the edge of the optic zone to avoid the displacement of some of the haptics towards the sulcus.
In case of posterior capsule tear, a 3-piece lens should be considered for implant in the sulcus if there is enough capsular support. These lenses have the advantage of thinner haptics and angled junction with the lens optic, allowing for a better adaptation to the sulcus than the single block lenses. The optic zone edge should be rounded instead of straight and marked as is the case of the AcrySof lens to reduce the pigment dispersion. If possible, the lens to be implanted in sulcus should have an optic zone of at least 6mm and a total length exceeding 13 mm in order to avoid lens displacements (21). It is possible that, even though the pigment dispersion may occur after sulcus implant of other single block acrylic lenses, this condition may be more evident due to its design in the case of implanting an AcrySof lens.
REFERENCES
-
Campbell DG. Pigmentary dispersion and glaucoma. A new theory. Arch Ophthalmol 1979; 97: 1667-72.
-
Woodhams JT, Lester JC. Pigmentary dispersion glaucoma secondary to posterior chamber intra-ocular lenses. Ann Ophtahlmol 1984; 16: 852-855.
-
Masket S. Pseudophakic posterior iris chafing syndrome. J Cataract Refract Surg 1986; 12: 252-256.
-
Pavlin CJ, Harasiewicz K, Foster FS. Ultrasound biomicroscopic analysis of haptic position in late-onset, recurrent hyphema alter posterior chamber lens implantation. J Cataract Refract Surg 1994; 20: 182-5.
-
Chang SHL, Lim G. Secondary pigmentary glaucoma associated with piggyback intraocular lens implantation. J Cataract Refract Surg 2004; 30: 2219-2222.
-
Iwase T, Tanaka N. Elevated intraocular pressure in secondary piggyback intraocular lens implantation. J Cataract Refract Surg 2005; 31: 1821-1823.
-
Chang WH, Werner L, Fry LL, Johnson JT, Kamae K, Mamalis N. Pigmentary dispersion syndrome with a secondary piggyback 3-piece hydrophobic acrylic lens; case report with clinicopathological correlation. J Cataract Refract Surg 2007; 33: 1106-1109.
-
Watt RH. Pigment dispersion syndrome associated with silicone posterior chamber intraocular lenses. J Cataract Refract Surg 1988; 14: 431-433.
-
Skorpik C, Menapace R, Gnad HD. Grasl M, Scheidel W. Evaluation of 50 silicone posterior chamber lens implantations. J Cataract Refract Surg 1987; 13: 640-643.
-
Uy HS, Chan PST. Pigment release and secondary glaucoma after implantation of single-piece acrylic intraocular lenses in the ciliary sulcus. Am J Ophthalmol 2006; 142: 330-332.
-
Wintle R, Austin M. Pigment dispersion with elevated intraocular pressure after AcrySof intraocular lens implantation in the ciliary sulcus. J Cataract Refract Surg 2001; 27: 642-644.
-
Woodhams JT, Lester JC. Pigmentary dispersion glaucoma secondary to posterior chamber intra-ocular lenses. Ann Ophthalmol 1984; 16: 852-855.
-
Pignalosa B, Toni F, Liguori G. Pigmentary dispersion syndrome subsequent IOL implantation in P.C. Doc Ophthalmol 1989; 73: 231-234.
-
Samples JR, Van Buskirk EM. Pigmentary glaucoma associated with posterior chamber intraocular lenses. Am J Ophthalmol 1985; 100: 385-388.
-
Mendez-Hernandez C, Fernandez-Barrientos Y, Fernandez-Vidal A, Martinez-de-la-Casa JM, Saenz-Frances F, Garcia-Feijoo J. Secondary pigment dispersion syndrome after in-the-bag AcrySof intraocular lens SN60AT implantation. Can J Ophthalmol 2008; 43: 120-121.
-
Boutboul S, Letaief I, Lalloum F, Puech M, Borderie V, Laroche L. Pigmentary glaucoma secondary to in-the-bag intraocular lens implantation. J Cataract Refract Surg. 2008 Sep; 34(9): 1595-7.
-
Rhéaume MA, Duperré J, Harasymowycz P, Thompson P. Pigment dispersion and recurrent hyphema associated with in-the-bag lens implantation. J Cataract Refract Surg. 2009 Aug; 5(8): 1464-7.
-
Kohnen T, Kook D. Solving intraocular lens-related pigment dispersion syndrome with repositioning of primary sulcus implanted single-piece IOL in the capsular bag. J Cataract Refract Surg. 2009 Aug; 35(8): 1459-63.
-
Micheli T, Cheung LM, Sharma S, Assaad NN, Guzowski M, Francis IC, Norman J, Coroneo MT. Acute haptic-induced pigmentary glaucoma with an AcrySof intraocular lens. J Cataract Refract Surg. 2002 Oct; 28(10): 1869-72.
-
LeBoyer RM, Werner L, Snyder ME, Mamalis N, Riemann CD, Augsberger JJ. Acute haptic-induced ciliary sulcus irritation associated with single-piece AcrySof intraocular lenses. J Cataract Refract Surg. 2005 Jul; 31(7): 1421-7.
-
Chang DF, Masket S, Miller KM, Braga-Mele R, Little BC, Mamalis N, Oetting TA, Packer M; ASCRS Cataract Clinical Committee. Complications of sulcus placement of single-piece acrylic intraocular lenses: recommendations for backup IOL implantation following posterior capsule rupture.