INTRODUCTION
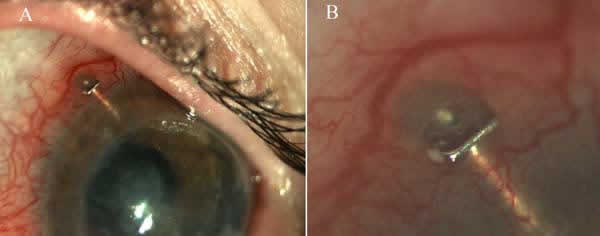
ExPRESS implants are a filtrating mechanism that maintains a permanent flow of aqueous humor in the subconjunctival and suprachoroidal spaces. These implants, made of stainless steel, have no valves and their penetration is limited by a distal flange and a proximal spur that prevents extrusion. The first ExPRESS device appeared in 1998, marketed by Optonol Ltd. The initial R-50 model was designed for insertion under the conjunctiva for chronic open angle glaucoma; subsequently, the P-50 model included an additional drainage perforation and a larger flange to prevent extrusion. At present, these implants are marketed by Alcon Labs. Initially, the implant was placed directly under the conjunctiva in a brief surgery of just a few minutes, although complications were detected together with frequent conjunctival erosions. Accordingly, Dahan and Carmichael (1) suggested a new approach, placing the implant under a scleral pad. This new technique is carried out in a similar way as traditional trabeculectomy, i.e., a subconjunctival incision is made on the base of the limbus and a pad comprising 50% of the overall scleral thickness. Before introducing the implant a pre-incision is made with a 27G needle and the ExPRESS device is introduced in parallel to the iris (figs. 1 and 2).
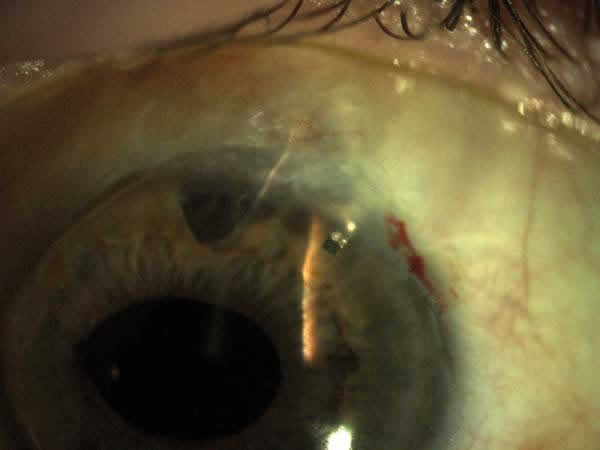
Fig. 1:
ExPRESS implant correctly located in the anterior chamber with an active3
filtration bleb in a patient with limbar insufficienty.
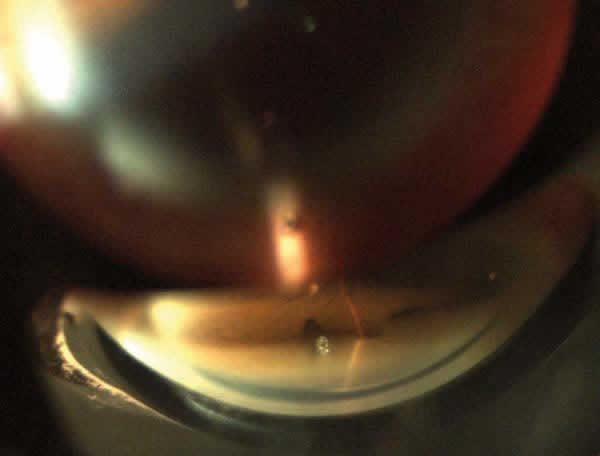
Fig. 2:
Gonioscopy view of an ExPRESS implant placed in the anterior chamber parallel to
the iris.
From a theoretical viewpoint, the ExPRESS implants have two main advantages: ease of insertion, which involves a significant reduction of surgery time, and a high degree of biocompatibility which prevents scar fibrosis, the most frequent cause of failure of filtrating techniques. Nyska et al (2) analyzed the histology of rabbit eyes submitted to ExPRESS implant surgery without finding signs of irritation or inflammation at 3 and 6 months, demonstrating their biocompatibility.
Since this new miniature implant was considered to be a reliable alternative to trabeculectomy, several studies have assessed a number of aspects such as efficacy, safety and side effects both in isolated filtrating surgeries and in combined surgery, or relative efficacy vis-a-vis other surgical techniques for glaucoma.
This literature review aims at analyzing the results described to date on the efficacy and post-surgery evolution of patients who underwent ExPRESS implants. To this end, we utilized the MEDLINE and EMBASE databases with the Pubmed and OVID SP search engines.