TECHNOLOGICAL UPDATES IN OPHTHALMOLOGY
Infrared Coordimetry. New ocular motor exploration test
PEREA J1, CABRERA Á2
1
Emeritus Ophthalmological Physician.
2 Orthoptist Nurse.
ABSTRACT
A new exploration procedure is presented for diagnosing, quantifying and following up specific ocular motility disorders: heterophoria, ocular palsy, restrictive syndromes, deviation incomitances and in general dynamic alterations of biocular imbalances. It has been named «Infrared Coordimetry».
The method applied is as follows: video-oculography with VOG-Perea device (1) placing in front of the eye lens of a color which is supplementary to the projected stimuli. The result was positive in all applications.
This test is considered by the authors to be nowadays the best way to study motor dynamic pathologies requiring bi-ocular dissociation when both eyes are lighted with infrared light.
Key words: Video-oculography, VOG-Perea, infrared coordimetry.
PRESENTATION
«Infrared coordimetry» is a test to be utilized in video-oculography, when bi-ocular light is infrared radiation (2). The large dicroic (transparent) lens placed in front of the patient eyes at 45º enables complete reflection of radiation impervious to the lens. A camera, located at the base of the device, simultaneously films the movements of both eyes in the proximity of the infrared (870 nm). In order to ensure this lighting, an infrared LED is placed under each ocular globe.
Said exploration procedure utilizes a red lens placed in front of one eye of a, which is supplementary to the green stimulus projected on the screen. In this way, the eye having a red lens in front of it does not see the stimulus and acts as if it were occluded even though its movement is recorded by the camera because the equipment is projecting infrared light on the eyes. The other eye is able to see the green stimulus and follows its movements. On the basis of Terrien-Quéré’s «Motor Equivalence Law», said the movements are consistent, Sino allergic and perfectly matching at the motor level the movements made by the other eye with the red lens in front of it.
«Infrared coordimetry» is the perfect procedure when assessing a patient with diplopia due to paresis or palsy as it avoids the confusion the patient may experience when maintaining both eyes uncovered because in this condition the patient sometimes doubts and even changes the fixation of the stimulus from one eye to the other according to the diplopic image he selects to focus on at any given time. On the other hand, this technique also assesses primary and secondary deviation.
Sensory dissociation produced by the inclusion of the red lens allows the device to be utilized for studying a broad range of pathologies.
INDICATIONS
The most important indications of «Infrared Coordimetry» are all ocular motility expirations in which it is necessary to disassociate one eye from the other.
Mainly:
• Study of Heterophorias (50 cases: 30 exophorias, 24 endophorias and 6 vertical phorias).
It allows diagnostic and quantification of phorias in all dire actions of the listing plane.
Study of strabismus (50 cases: 20 endotrophies, 12 exotrophies, 10 alphabetic syndromes, 8 adduction elevations). In addition, it assesses angles, alphabetic syndromes, muscular hypo- and hyper-function in all diagnostic positions when it is necessary to carry out to the study in maximum dissociation
• Fixation incomitances (12 cases). Angle value of strabismus focusing each eye alternatively in all possible directions.
• Version incomitances:
Simple version test (focusing each eye alternatively)
Static version test with occlusion (Quéré).
Test seeking the stop sign (Corcelle). Prismatic kinetic test (Cüppers).
• Closet convergence point, focusing one eye or the other (30 cases)
• Study of paresis and oculo-motor palsy (23 cases: 12 superior oblique palsies, 5 superior rectus palsies and 6 lateral rectus palsies).
As discussed above, this test requires previous practice.
The main advantage in the exploration of ocular-motor palsies with video-oculography when compared to the Lancaster screen include its short test duration, its validity for patients with anomalous retinal correspondence, greater precision, real time test follow-up, graphic record of movements, allowing for simultaneous comparison with ocular movements, visualization of the coordimetric diagram and of the oculo-motor threshold value and that it can be performed even when the angle is significant, among others.
• Restrictive syndromes (21 cases, 8 Duane Type 1 syndromes, 4 Duane Type II syndromes, 5 Duane Type III syndromes, 4 Brown syndromes).
The purpose is the same as in the previous section.

Fig. 1: VOG-Perea equipment.
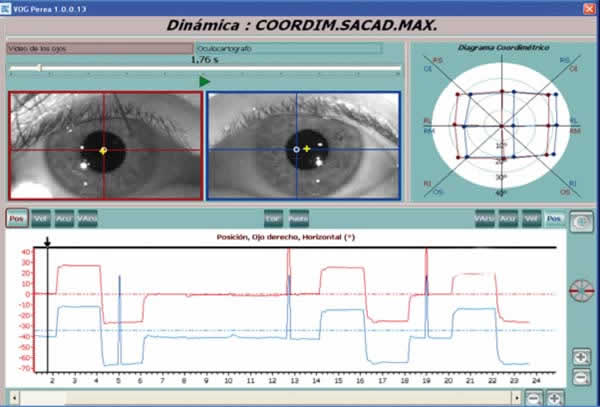
Fig. 2: Exophoria 5.5º LE.
Infrared coordimetry: Red lens in front of LE.
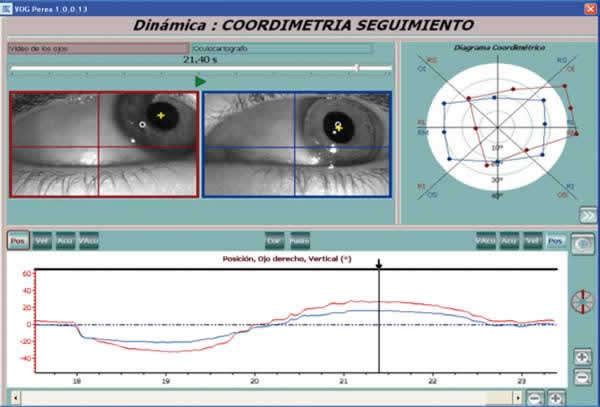
Fig. 3: RE inferior oblique
hyperfunction (11°) due to palsy of the homolateral antagonist (superior
oblique). Infrared coordimetry: Red lens in front of RE. Oculoscope and
Oculograph show hyperfunction of the RE inferior oblique. The Coordimetric
diagram shows said hyperfunction and IV right pair palsy. The ascending portion
of both curves (seen in the Oculograph) reveals «rhythmic waves » which are
specific to congenital endotrophy when the dominant eye abduces, (in this case
the LE).
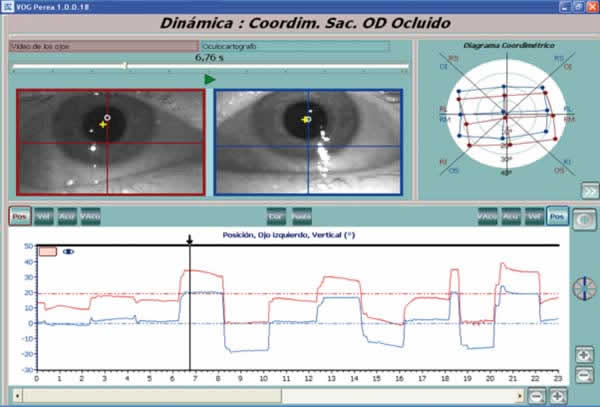
Fig. 4: RE upper rectus palsy.
Infrared coordimetry: Red lens in front of RE, showing limitation in RE
elevation and hyperfunction of the homolateral antagonist.
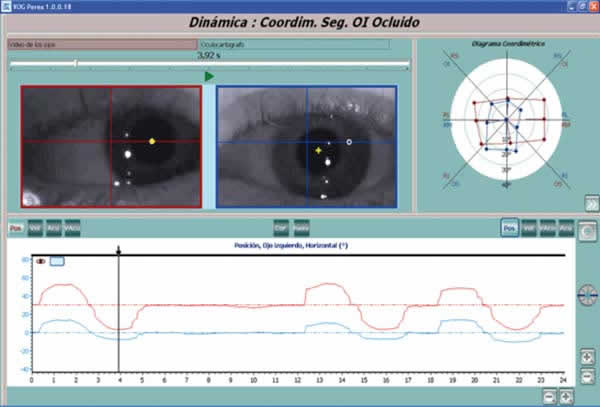
Fig. 5: Duane syndrome Type III.
Infrared coordimetry: Red lens in front of LE, evidencing adductor and abductor
limitation, clearly seen in the Coordimetric Diagram.
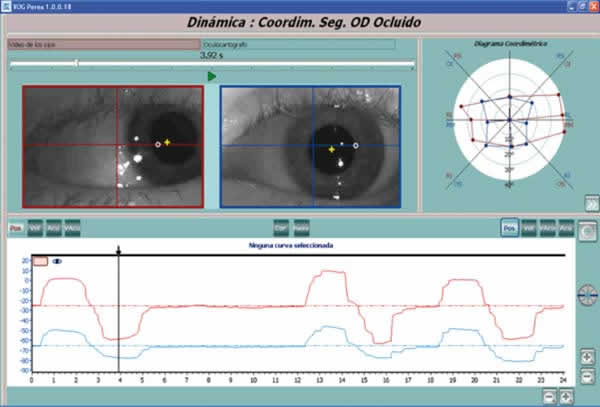
Fig. 6: Duane syndrome Type III
(case shown in Figure 5). Infrared coordimetry: Red lens in front of RE. The
Coordimetric Diagram shows the larger amplitude of the RE in accordance with
secondary deviation which must be larger than the primary deviation.

Fig. 7: Duane syndrome Type III
(case show in Figure 5). The Oculograph plot shows orthotopia in frontal
fixation (indicated by black arrow),and e incomitance in dextroversion and, more
importantly, in levoversion. Infrared coordimetry with Red lens in front of LE.
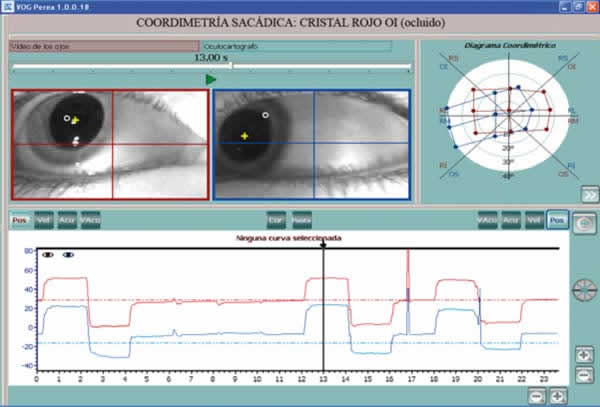
Fig. 8: Brown syndrome. In
the supradextroversion movement the LE hardly goes beyond the middle line. This
test was made with infrared Sacadic Coordimetry (Red lens in front of LE).

Fig. 9: LE lateral rectus palsy.
A 3.5° limitation of the LE in levoversion can be appreciated. Exploration with
Infrared coordimetry (red lens in front of LE).
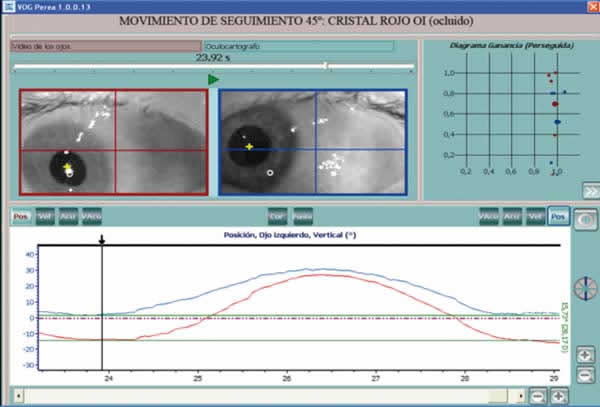
Fig. 10: Left IV pair palsy.
Following movement at 45° in the direction of action of LE superior oblique
(infradextroversion), made with Infrared coordimetry (red lens in front of
LE).The difference in height at that time was of 15.73°. As shown by the
Oculoscope, the LE does not go beyond the middle line.
CONCLUSIONS
The results of Infrared coordimetry has been positive and the objectives were achieved in all performs assessments. It is obvious that this result refers to patients with poor cooperation, as is the case with any ophthalmological exploration test.
REFERENCES
-
Perea J. Estrabismos. Toledo: Artes Gráficas Toledo; 2008; 293.
-
Perea J. Fisiopatología del equilibrio oculomotor. Madrid: Brosmac S.L; 2011; 241 y 372.
(Literary Search)
Search date: March 26, 2011. Publication date limits
were not set. Bibliographic references cited below were obtained from the
National Library of Medicine’s PubMed database and The Cochrane Library. Key
words: videooculography, video-oculography, infrared lighting and infrared
coordimetry. No language restrictions were set. Published references unrelated
to ocular motility and its direct application to ophthalmology were excluded. On
the basis of these criteria, no written precedent has been found in world
medical literature.