CAPÍTULO 24 LOW-TECH DETECTION TEAR FILM RELATED Maurizio Rolando, Angelo Macri |
| Especially in early cases, the detection
of tear film related pathology of the ocular surface during routine clinical eye
examination, is not always easy and straightforward. Therefore, a number of specific tests such as Schirmer Test, Fluorescein and Rose Bengal Staining, Tear Ferning Test, Conjunctival Impression Cytology, etc. have usually to be added to the current eye examination to fomulate the correct diagnosis (Farris 1983, Goren 1988, Rolando 1983b, Rolando 1985). Unfortunately the adjunct of these specific tests to the routinely used series of clinical ophthalmologic examinations, results time expensive and it is often neglected by the general ophthalmologist. This leads to the consequence that the diagnosis of tear fllm disorders by the general ophthalmologist is not as frequent as it could be, with the obvious consequences for the well-being of the patients. As always in medicine, the basis for a correct diagnostic approach to a disease are: an intelligent collection of symptoms (anamnesis) and a careful observation. While there is a rather standardized way for collecting the ocular surface signs, the collection of typical symptoms and their relevance as a diagnostic indicator has not been established yet. The definition of dry eye as a disorder of the tear film due to tear deficiency or/and tear evaporation which causes damage to the ocular surface and is associated with symptoms or ocular discomforts, clearly underlines that in the manifestation of the disease the subjective symptomatology has a relevant part.
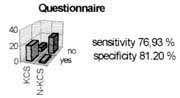
THE DRY EYE QUESTIONNAIRE We developed a questionnaire based on the symptoms and the history which are more frequently reported by dry eye patients. In order to select the three most frequent and specific symptoms for dry eye, 20 patients with tear film related ocular surface diseases and 20 patients with non tear film related ocular surface diseases have been selected. From these patients on the basis of a list of dry eye symptoms present on the ophthalmic literature (Goren et al 1988) the three symptoms with the best sensitivity and specificity detecting dry eye among normal eyes and eyes with different eye surface pathology were selected, and identified as fundamenta/ symptoms, while the remaining were considered accessory symptoms (table 1). Our questionnaire, largely derived from McMonnies questionnaire (Rolando et al 1983b) consisted of five main sections: apart of the already mentioned fundamental symptoms (section 1) and accessory (section 2), included fundamental and accessory symptoms time relations, environmental stress condition related symptoms (section 3), need of topic therapy (section 4), use of systemic drugs (section 5) and presence of systemic diseases (section 6) able to produce or associated with dry eye conditions. Table 2 describes the details of the questionnaire. The overall evaluation of the answers can give a reasonable understanding of the origin of ocular surface disease, but a quantitative scoring will give more precise information on the level of risk that the patient has to be primarily affected by a tear film related ocular surface disease.
SCORING SYSTEM For every symptom considered in the questionnaire a score is given according to an analogic semi-quantitative presentation, composed by a line with a ruler graded zero to nine on which the patients, with the help of a staff member, should mark the entity of his/her symptomatology; in this way a sub-total score for each symptom was obtained. The total score for each patient was calculated by the sum of the single sub-total scores except for the fact that the main symptoms are scored on the basis of the sum of the sub-lotal scores, while the accessory symptoms are scored by the sum of the sub-total scores divided by three. In the sections three to six, each positive answer to any of the questions scored 1. The questionnaire was applied to a population of 268 patients including a group of 112 healthy normals (age = 62+/- 18, female/male ratio (f/m) = 2.7), a group of 43 ophthalmic patients with no ocular surface diseases (no-osd) (age = 67±12, f/m =2), a group of 70 non tear film related ocular surface diseases (osd-no kcs) (age = 53±9, f/m=2.05) and a group of 43 patients with tear film related ocular surface diseases (kcs) (age = 56±13, f/m = 6.1). The sensitivity and speciflcity of the questionnaire as a whole in separating the KCS patients from the other groups were tested. By means of the study of the area under the ROC (Receiver Operator Characteristics) curves, the score of 17 was then identified as the one with the best ability in separating dry eyes from normal and other pathologic eyes. Figure 1 reports the frequency distribution of symptoms in the four groups of subjects considered; Table I shows the sensitivity and specificity of each single symptom in separating dry eyes from the other groups;
Figure 2 shows the best area under ROC curve indicating the best compromise specificity and sensitivity, obtained when the questionnaire total score of 17 was used as a separator between dry eye and non dry eye patients.
The use of a systematic approach in symptoms collections in dry eye is in many ways critical. It is a common clinical experience that very often the dry eye patients will not designate, if not explicitly asked the occurrence of a precise symptom, while he will generally complain of eye discomfort. A characteristic of dry-eye patients is the frequent incongruence between the level of ocular surface damage and the symptomatologic complaint. There are patients with minimal ocular surface involvement with high level of complaint in front of a large number of patients with definite typical conjunctival and corneal damage who do not have a spontaneous declaration of symptoms except an undefined feeling of discomfort. These patients only if asked for will tell the presence of specific typical symptoms. Furthermore many patients if not precisely asked will mismatch symptoms. Burning and pain and foreign body sensation and hitching being the more frequently confused. The ocular surface has receptors for touch, heat and pain. Subjective symptomatology is the result of activation of these receptors. As it has been recognized, symptomatology is a main point in diagnosis of Keratoconjunctivitis Sicca, which has typical subjective signs and typical time relation occurrence. Our questionnaire showed an interesting ability to separate dry eyes from non tear related ocular surface diseases, which will prove useful in the clinic, especially in controversial cases were the ocular surface pathology is mixed because of the presence of concurring diseases, or in early cases were the objective symptomatology is not patent. Systematic and ordered evaluation of the prevalence and the significance of a number of subjective symptoms could be of great help in setting diagnostic networks for many ocular surface diseases. A validated questionnaire could be a useful tool for population screening for dry eye as well as a useful diagnostic parameter to be used in the clinic. TABLE 2 SINGLE TEST
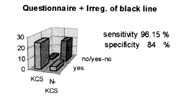
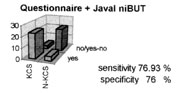
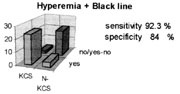
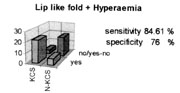
TWO TESTS ASSOCIATED
CLINICAL OBSERVATION Together with symptoms collection, there is a number of signs and characteristic aspects of the ocular surface in tear film related diseases which could be used in a clinical setting as indicators of a tear film problem or as a hint toward the need of a complete, more complex and time consuming diagnostic procedure. A localized hyperemia confined in the interpalpebral fissure, the presence of a lip like fold in the inferior conjunctiva, the irregularity of the black line and a "rapid deteriorating image at Javal keratometry" are easily collected clinical signs, available to every ophthalmologist in a routine practice.
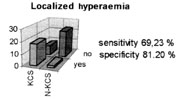
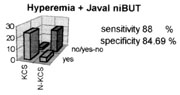
LOCALIZED HYPEREMIA A "conjunctival hyperemia localized inside the interpalpebral fissure" is a rather frequent presentation of early tear film related ocular surface patology, when this is not mixed with other more diffuse surface inflammations The appearance of interpalpebral fissure confined hyperemia is a clear suggesting that the protection of the ocular surface, in the area not already protected by the lids has failed. The ocular surface protection between blinks is demanded to the tear film and its failure should consequently implicate that qualitative or quantitative changes are occurring in the tear film, which impair its protective function or are at the origin of these localized changes. Epithelial changes to the interpalpebral fissure are typical of early Keratoconjunctivitis sicca. The increased tear water evaporation rate, typical of tear film instability and caused by the consequent altered spreading or by an inadequate production of the lipid layer, has been reported to be at the basis of this phenomenon. When the lacrimal gland secretion cannot keep the pace with such excessive tear evaporation, both because of an absolute reduction in tear flow (absolute tear hyposecretion) or because the tear flow, theoretically sufficient for normal ocular surface needs, cannot satisfy the increased request caused by environmental conditions, bad blinking habits or contact lens wearing (relative tear hyposecretion) epithelial changes and inflammation of the exposed ocular surface can occur. The high rate of water evaporation causes water loss from the tears and increased electrolyte concentration on the ocular surface, resulting in localized hyper-osmolarity of the tear film and histologic changes of corneal and conjunctival epithelia.
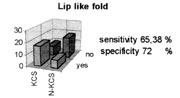
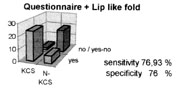
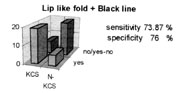
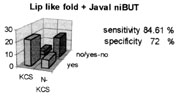
LIP LIKE FOLD OF THE INFERIOR CONJUNCTIVA The presence of a "lip like fold of the inferior conjunctiva" (Rolando et al 1983a) has been suggested to be a rather sensitive and specific (% sensitivity and % specificity) sign of tear film related ocular surface problems. It can be recognized by observing the shape of the bulbar conjunctival layer in correspondence to the inferior lid margin. When present, it can be recognized as a real fold of the conjunctival sheet in proximity of the inferior tear meniscus. Such a fold can be just barely visible at the temporal corner, (grade 1), clearly visible in the temporal bulbar conjunctiva (grade II) or visible also in the conjunctiva corresponding to the inferior corneal limbus (grade III).
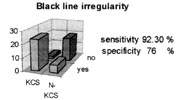
IRREGULARITY OF THE BLACK LINE The black line (Rolando et al 1990) is an easily collectable landmark of the tear fluid volume and the evaluation of its morphology can be used as a diagnostic hint. When the tear film is colored by means of a fluorescein strip, under Wood light illumination a distinct black line stands out on the ocular surface, separating the yellowish precorneal tear film from the adjacent tear meniscus. Albeit the phenomenon occurs in proximity of both the superior and the inferior tear menisci usually, the clinical evaluation is made on the inferior black line, which is easily and instantly examined at the slit lamp. Considering its genesis, the black line can be considered as a linear area of localized thinning, caused by the traction exerted on the tear film by the concave thirsty menisci which are originated by the distribution of the tear fluid in the angle formed by the lid border and the convex surface of the eye. Up to a certain limit, the thicker are the tear film and the meniscus, the stronger is the force of traction exerted on the tears by the meniscus and, as a consequence, the thinner and more regular will be the black line. In presence of low volumes of tears and of a scanty tear meniscus, the centrifugal traction exerted on the tear fluid spread on the ocular surface will be very low and the black line will appear wider and irregular. The presence of an irregular black line should be considered a sign of decreased tear fluid volume available for the ocular surface. The only change needed in the routinely eye examination is that fluorescein tear staining should be performed before and not after the instillation of the topical anesthetic during intraocular pressure measurement.
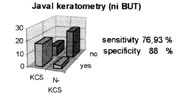
QUALITY OF JAVAL KERATOMETRY Javal keratometry is based on the reflex of light from the surface of the precorneal tear film (Gilbard et al 1979). If the precorneal film because of quantitative or qualitative cannot spread regularly on the corneal surface or if it has significant thickness irregularities, the light reflex will result irregular and of low quality, and can be easily detected through the optic system of the instrument. In a way this is similar to tho functioning of the non invasive Break-up time (ni-BUT), probably with a lower sensitivity since the ni-BUT explores all the precorneal surface while the Javal keratometer measure only relatively small areas of the cornea (approximately 3 mm in diameter) and will be able to detect only tear film problems occurring in this small central area. A rapid deterioration of the image at the Javal keratometry will reflect the rapidity of changes in the quality of vision of the eyes with tear film problems which are reported to have decreased spatial contrast sensitivity when compared to normals. Corneal shape irregularities such as keratoconus or scars, as well as the presence of ulcerations, punctate keratitis, etc. which will affect the quality of Javal keratometry in dependent or independent way from tear film distribution and stability should be considered and ruled out.
TESTING THE DIAGNOSTIC POWER OF LOW TECH TESTS In order the evaluate the sensitivity and the specificity of this clinical presentation in the diagnosis of a tear film related disease, a population of patients with ocular surface disease was evaluated. Such a population included 26 subjects with diagnosis of KCS assessed on the basis of: Presence of at least 2 positive results among
These patients had: typical signs and symptoms of ocular surface disease but negative results to the dry eye tests:
METHODS All the patients had to refrain from using any topical therapy for at least 12 hours before the visit and were evaluated by means of:
The sensitivity and specificity of the questionnaire (positive if score >17), of the conjunctival lip like fold, of the irregularity of the black line and of the observation of tear surface reflection at Javal Keratometry, alone and in association, in detecting dry eyes ( in respect to the classical methods used for diagnosis of KCS) were then evaluated.
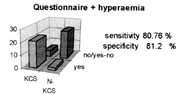
RESULTS As a single test the presence of irregularity of the black line had the best compromis between sensitivity and specificity (92% sensitivity and 76% specificity) in diagnosing dry eye conditions. Among the possible associations of clinical presentations, the associations Questionnaire + Irregularity of the black line and Localized hyperemia + Irregularity of the black line show the best compromise between sensitivity and specificity in diagnosing dry eye conditions. Dry eye diagnosis is the result of a composite approach to history, subjective and objective symptomatology of the patient and is often reached after a quite complex, time consuming sequence of tests. Easy and quick to be performed tests are loved by ophthalmologists and patients and have more chances to be used. Low cost tests, easy to perform during a routine eye examination such as dry eye questionnaire (Gilbard et al 1978, 1984), research of a lip like fold at 6 o´clock, research of hyperemia localized into the interpalpetral area, research of black line irregularity and irregular targets at Javal keratometry (ni-BUT) have a nice sensitivity and specificity in diagnosing dry eye conditions. They are easily learned and mastered by any ophthalmologist, their use will add no substantial extra time to the examination schedule and can provide further information about tear film and ocular surface conditions. Unfortunately no single test has the ability of providing a sure diagnosis of dry eye, but can suggest the need of further investigation and when necessary, in suspect cases, the diagnosis of KCS should be assessed by performing the classical dry eye tests. |