TECHNOLOGICAL UPDATES IN OPHTHALMOLOGY
Applications of robotic surgery in ocular surgery
BARRETO GALEANO A1, NIEVA PASCUAL I1, NAVAS SANCHEZ A2, MATEOS VICENTE C1
Ophthalmology Service. Gregorio Marañón
Hospital. Madrid.
1 Graduate in Medicine and Surgery.
2 Graduate in Medicine and Surgery. Retina and Vitreous Unit.
RESUMEN
In the ophthalmological field, the Da Vinci surgical system could provide important benefits in ergonomic improvements, tremor filtering and strength distribution compared to standard ocular surgery. This article reviews current ocular surgery applications as well as its advantages and disadvantages.
Key words: Da Vinci surgical system, ocular surgery.
PRESENTATION
The Da Vinci surgical system, developed by Intuitive Surgical, is a surgical robot designed to facilitate minimally invasive approaches in complex operations. The name is a tribute to the artist who built the first robot.
Da Vinci is a computer-assisted surgical robotic platform, i.e., it does not perform operations autonomously and requires the control of an expert surgeon. Basically, the system consists in an ergonomic console comprising a display screen from which the surgeon remotely controls the platform and interacts with it by means of two control levers and two pedals and a series of four articulated electromechanical arms (figs. 1 and 2).
In parallel, the sophisticated equipment digitizes with extreme precision the movements of the surgeon’s hand in the console which, in real time, are faithfully reproduced by the arms of the robot, correcting tremors and reaching locations of impossible access to the human hand due to its extremely reduced diameter.
The equipment comprises three components:
– The surgeon console: the command centre of the Da Vinci system. The surgeon is located outside of the sterile field and controls the 3-D endoscope and the Endowrist instruments through two manual controls and two pedals. The system interprets the surgeon’s movements and translates them to scale in real time and with great precision to the instruments.
The patient trolley: this is the surgical component of the Da Vinci system. Its main function is to sustain the arms for the instruments and the 3-D endoscopic camera. This system utilizes a control centre technology that allows the manipulation of instruments and endoscopy only in the selected area, exerting the minimum pressure on adjacent tissue.
The operation of the robotic arms of the Da Vinci system is truly amazing (figs. 1 and 2). The first two arms, representing the left and right hand of the surgeon, handle a number of surgical instruments which were specifically designed for the robot, what is known as EndoWrist, while a third arms which includes an endoscopy with two sophisticated high-resolution 3-D video mini-cameras allows the internal visualization of the entire operation. For the surgeon it’s like immersing the head into the patient’s body.
If the surgeon needs a higher degree of detail of the are to be intervened, the system can increase up to 20 times the original image, or automatically enhance a given area without a perceivable loss of resolution. In addition, said third arm allows the surgeon to easily change, move and rotate the visual field of the endoscopy, which represents a huge advantage for the surgeon.
Finally, the fourth arm of the machine carries out the tasks of a surgical assistant, separating tissue during the operation or suturing with bewildering ability the wounds of the incisions (fig. 1).

Fig. 1: The Da Vinci surgical equipment.
The user of the patient trolley works in the sterile zone, assisting the surgeon with the replacement of instruments and endoscopies.
– Visualization trolley: it allows all the operating theatre personnel to follow the operation in real time (1) (fig. 2).

Fig. 2: The Da Vinci surgical robot.
EndoWrist is the name given to mini-surgery instruments specifically manufactured for the Da Vinci system and the actual performers of the intervention. Their carefully planned and intuitive design allow a full range of movements which perfectly imitate the movements of the surgeon’s wrists. Even more, with seven types of movements and 90-degree articulation, EndoWrist is able to perform maneuvers with a degree of ability exceeding that of the human hand. The EndoWrist line movements are based on internal cabling simulating the human tendons, includes a large range of tools like forceps, needles, scissors, scalpel, electrocauterium, etc. which allow the team to dissect, suture or manipulate the most delicate tissues with a high degree of precision (1) (fig. 3). The instruments, manufactured in diameters of 5-8 mm, must be replaced every 10-12 interventions in order to preserve their quality. In addition to its multiple use feature, the EndoWrist instruments are designed to allow the surgeon to maintain his/her skill and also to provide a broader range of movements than the human hand.

Fig. 3: EndoWrist (surgical microinstruments).
By providing enhanced ergonomic comfort, improved visualization of the surgical field, greater precision and skill, the EndoWrist instruments enable complex procedures with minimally invasive approaches (2).
USE IN GENERAL SURGERY
The Da Vinci system was originally designed to improve traditional laparoscopy in which the surgeon uses manual instruments while standing, guided by a camera that projects the image to a 2-D screen.
The Da Vinci system was authorized by the FDA for laparoscopic general surgery in 2000. At present, its use is approved for laparoscopic procedures for digestive, urologic, gynecologic, ENT and cardiovascular procedures. The following operations can be performed successfully:
-
Radical prostatectomy, pyeloplasty, cystectomy, radical and partial nephrectomy, urethra reimplantand pelvic floor reconstruction.
-
Simple and radical hysterectomy, myomectomy and sacrocolpopexy and anexectomy.
-
Colecistectomy, Nissen funduplicature, Heller myotomy, sigma and rectum neoplasiae, bariatric surgery, gastric bypass, splenectomy and intestinal resection.
-
Mitral and tricusp valve repair, interauricular communication closure, cardiac ablation, aortic-coronary bypass and thymectomies.
-
Mediastinotomy, thoracotomy, thoracoscopy and mediastinoscopy.
-
Resections in oral-pharynx, larynx, hypopharynx, mouth floor and oral cavity.
-
Resection of benign and malign tumors classified as T1 and T2 (1). Advantages: it allows improved recovery for the patient as the incisions are of minimum size, less anesthesia is needed, infections are reduced as well as blood, loss, post-ophthalmological pain and scars are much smaller. All this ensures faster recovery and shorter hospital stays. In addition, it will soon be standard practice to manage these robots remotely (telesurgery) so we will be able to receive the attention of the very best surgeons in the world for each specialty.
In Spain, the Da Vinci system also enjoys a great reputation in the community of world class surgeons, even though the cost of the system amounts to about 1.5 million Euros.
USE IN OCULAR SURGERY
Classical ocular microsurgery is performed using a surgical microscope. The ocular structures which are anterior to the vitreous are intervened under direct vision whereas other structures in the posterior regions such as the retina and vitreous are intervened utilizing a special lens system (3).
Robotic surgery is potentially an ocular surgery mode which is not yet established as a routine procedure.
The Da Vinci system provides 3-D stereoscopic vision, a crucial requirement for ocular surgery, with three slave robotic arms which can be equipped with instruments having the necessary freedom of movement similar to the articulations of the wrist (4).
The operator is provided with an excellent depth of images and structures, with one of the main advantages being the ability to improve on fine movements of great precision with minimization of tremor (2).
Utilizing his hands, the surgeon retains master control at a comfortable distance and position. At present, microforceps are graded for sutures of up to 7/0, which means that new materials designed for finer sutures would be even more precise (1).
The use of robotic ocular surgery is not fully explored to date. The benefits it could provide regarding ergonomy, scale of movements, filtering tremor and strength distribution are important vis-à-vis standard ocular surgery. However, the integration of robotic ocular surgery still has drawbacks such as the high cost of the equipment, the need to develop specific instruments and the improvement of the optic system as it is not yet possible to match the optic quality of the conventional microscope for intra-ocular procedures (5).
To date, publications include data obtained from procedures carried out mainly in pig models, with successful corneal sutures (figs. 4 and 5), penetrating keratoplasties or epiretinal membrane peeling. However, there is a lack of sufficient experience on humans.

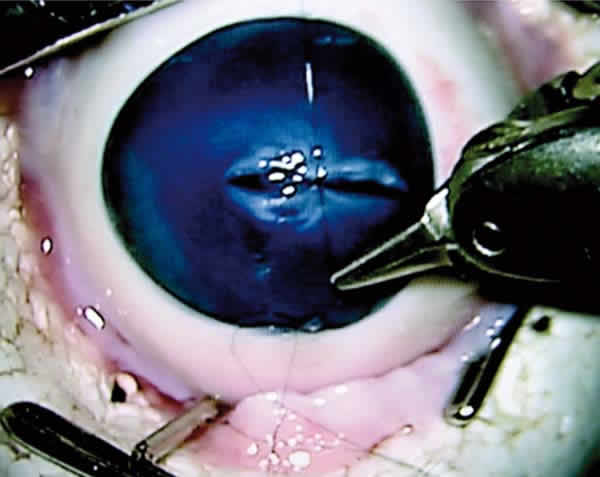
Figs. 4 and 5: Corneal suture.
The robust research program of the Robotic Surgery Centre is focused on the quest for safety and innovative applications for robotic technology. Measuring and analyzing the results of robotic surgery is an advantage against open surgery, in addition to being beneficial for patients.
Published data give rise to promising applications for robotic surgery which will lead to developments in cataract, vitreous and retina surgery in the future.
REFERENCES
-
Tirbas A, Mango C. Robotic ocular surgery. Br J Ophthalmol 2007; 91: 18-21.
-
Bourgel JL. Robotic microsurgery: Cornea transplantation. Br J Ophthalmol 2009; 93: 72-75.
-
Hubschman JP, Bourges JL, Choi W. The microhand a new concept of microforceps for ocular robotic surgery. Eye(Lond) 2010 feb 24; 364-367.
-
Bourges JL. Assesment of a Hexapod Surgycal System for robotic micro-macro manipulations in Ocular Surgery. Ophthalmic Res. 2010; 46: 25-30.
-
Bourla DH, Hubschman JP. Feasibility study of intraocular robotic surgery with the da Vinci surgical system. Retina 2008; 28: 154-158.