TECHNOLOGICAL UPDATES IN OPHTHALMOLOGY
Exploration of vergences with video-oculography
PEREA J1, ZATO MA2, CABRERA MA3
1
Emeritus Ophthalmologycal Physician. Ocular Motility Research Unit of the Health
Service of Castilla-La Mancha (SESCAM).
2 Professor of Ophthalmology. Instituto de Ciencias Visuales
(INCIVI).
3 Orthoptist Nurse.
ABSTRACT
The authors describe the way in which, in their view, vergences should be explored, showing the disparity between conventional procedures and video-oculography. A study was made utilizing VOG Perea on 21 patients with significant astenopic disorders who were considered normal with conventional motor exploration methods. The study protocol developed by the authors identified 6 patients with convergence insufficiency.
Conclusion: Current methods are obsolete. Once again video-oculography demonstrates that it is the best technique for detecting vergence pathology and for following up the results of orthoptic therapy.
INTRODUCTION
Vergence movements are disjunctive movements in response to disparities in visual stimuli on both retinas, placing the images of both eyes in normal retinal correspondence to avoid diplopia. Accordingly, the individual captures, analyzes, understands and memorizes spatial objects in the environment at different distances, producing dynamic and static convergence or divergence of the ocular axes. Consequently, the vergence function has a dual aspect: kinetic and static. Vergencies ensure the reciprocal balance at all distances, from the infinite to the near convergence point (1). These are the fundamental and basic movements of binocular vision which, in daily life, combine with version movements (saccadic accompanying movements and reflex displacements dependent on the vestibulo-ocular and optokinetic systems).
Currently, examinations are being carried out by means of guided vergences (2) and prismatic vergences (3). Both procedures are very old and artificial and do not match the usually performed convergence and divergence movements. Individuals in actual situations never converge or diverge with vergence following movememtns or static vergences utiloizing prismatic lenses.
Vergences should be analyzed by means of physiological procedures. At present the authors are utilizing the refixation vergence adapted to video-oculography (applied by Maurice Quéré through Electro-oculography), and sustained vergence, which has been included directly in the study protocol. The former due to being a rapid disjunctive movement which, combined with saccadic movements, represent the usual form of directing the gaze from one side to the other in order to capture an impression to immediately convert it into a perception. The latter due to the significant interest of this static vergence condition to explain persistent near vision astenopic disorders, the most frequent action of which is reading and working in professions requiring extended near vision periods such as watchmakers or engravers.
MATERIAL AND METHOD
a) Sample: 21 patients with significant subjective clinic for astenopic disorders in near vision. In the overall sample, 5 emmetropic and 16 ametropic patients were identified, with the following refractive defects:
Emmetropic: 5.
Myopic: 5.
Hypermetropic: 6.
Simple myopic astigmatism: 3.
Complex myopic astigmatism: 2.
Non-anisometropic or anisometropia under 1.50 D.
All the patients exhibited normal ocular transparency, normal ocular fundus and absence of relevant general or ocular pathology.
Visual acuity of one in both eyes with or without correction in emmetropic patients. Visual acuity was checked utilizing the finest discrimination power with maximum contrast between a test and its background. The minimum legible or contour acuity was utilized according to the morphoscopic visual acuity criterion. The applied test was the Raskin «E» test (measuring with white light and black tests over white background). Vision was exercised monocularly (in one and the other eye) at 5.5 metres (to provoke minimum accommodation).
The presentation background luminance was 200 cd/m2 with ambient luminance of 15%.
The optotype scale progression mode was geometric.
Normal contrast sensitivity. This assessment was made in pure luminance utilizing only black and white stimuli. The aim of this assessment was to obtain qualitative and quantitative data of the various frequency analysis channels. The normality criterion was based on the match with different spatial frequencies. The examination was made with Metrovisión and Roland Consult devices, both computer assisted.
The motor study revealed orthotropia with cover test. Guided and prismatic vergences also exhibited absolute normality. Binocular vision was normal with stereoacuity values of 30 arc seconds or better, upon Randot-test and Frisby.
b) The study was alwasy performed by the same orthoptist.
c) The examination equipment was the VOG Perea video-oculograph.
Fig. 1: Examination with the VOG
Perea device.
RESULTS
Despite normal values shown by «guided vergences» and prismatic vergences, video-oculographic examination detected:
-
2 patients with pathological «refixation vergence» (one also exhibited «sustained vergence« disorder).
-
4 patients with pathological «sustained vergence».
Illustrative graphs are included below (figs. 2-10).
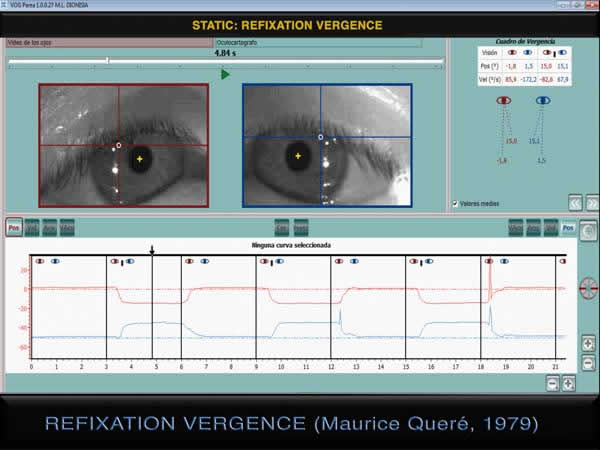
Fig. 2: Normal refixation vergence.
The patient gazes at a stimuli at 1.00 m and subsequently at 0.13 m. The figure
represents a convergence movement. This sequence is usually repeated only five
times because it is a tiring test.
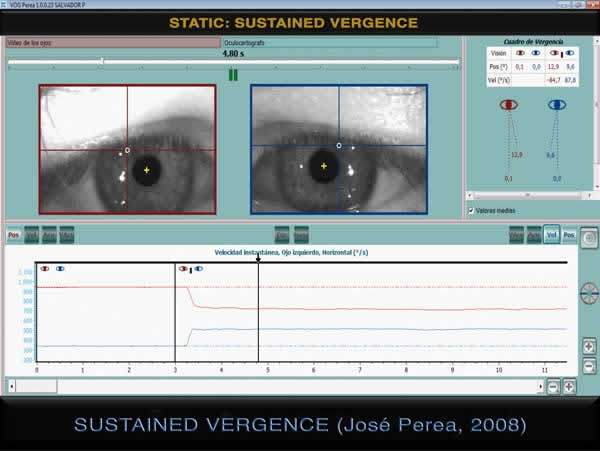
Fig. 3: Normal sustained vergence.
The patient gazes at a stimuli at 1.00 m and subsequently at 0.13 m., remaining
in this position for 35 seconds.
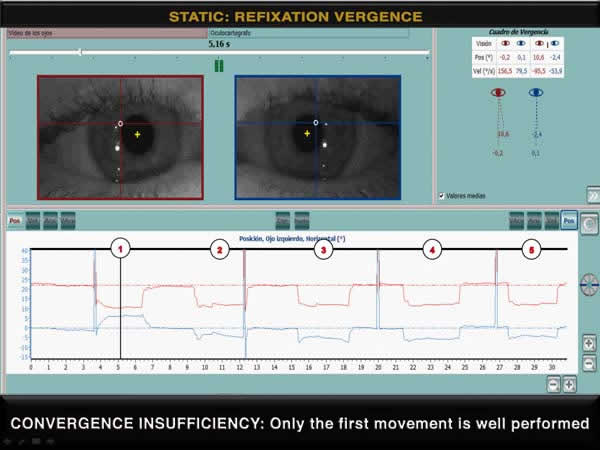
Fig. 4: convergence is normal only
in the first movement. The insufficiency appears as of the second movement
(shown in the oscilloscope and the oculograph) and persists in the 3 following
movements. Guided and prismatic convergences appeared normal. The figure depicts
the first movement, the only normal one.
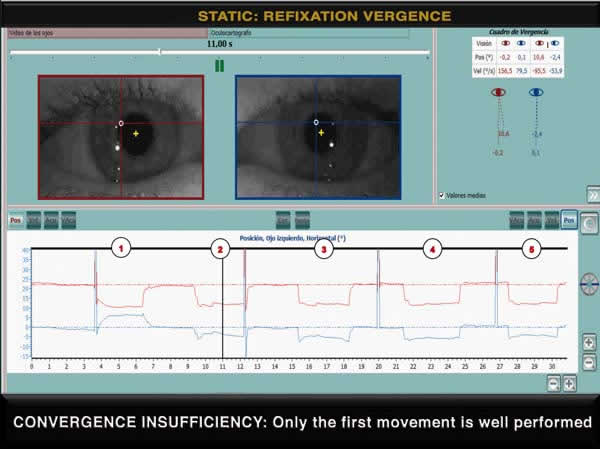
Fig. 5: Second movement of the
patient shown in the previous figure, clearly depicting convergence
insufficiency. The LE is led to abduction in «paradoxical version».
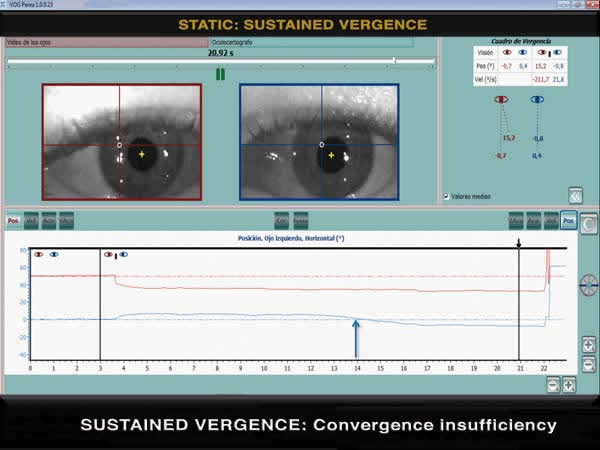
Fig. 6: Oculograph shows normal
convergence up to the time marked by the blue arrow, when convergence fails as
shown by the change of direction of the blue line which illustrates the LE
movements. The vergence instant of the figure (20.92s) is marked by the black
arrow and depicts LE insufficiency.
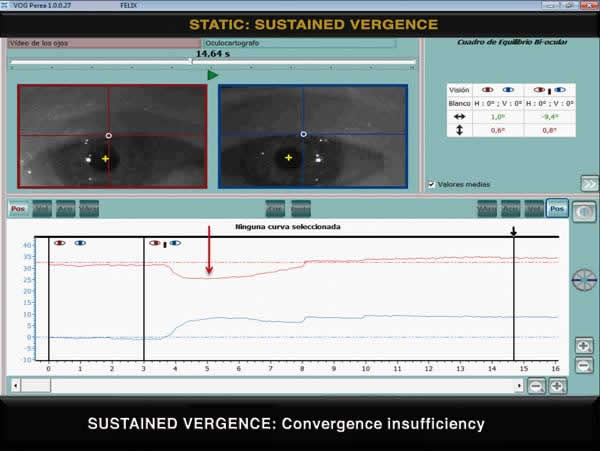
Fig. 7: Another convergence
insufficiency case. Here, the right eye goes to abduction at the time marked by
the red arrow.
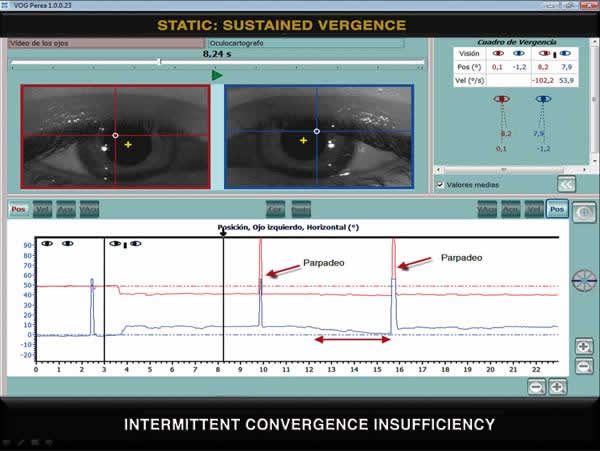
Fig. 8: The space shown by the
double red arrow for the LE (blue line) representes the claudication of this eye
in order to maintain convergence.Subsequent immediate blinking is a «refresher»
enabling recovery, as show by the line returning to normal values.
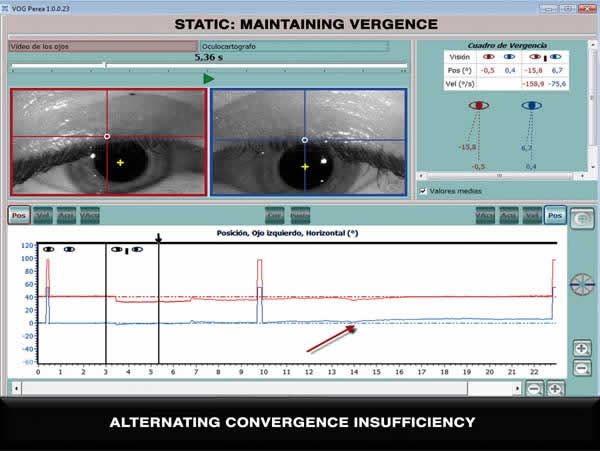
Fig. 9: Beginning with LE
insufficiency (blue line), at the point shown by red arrow it reverts and takes
control. At this point the RE (red line) depicts insufficiency (see oculograph).
The figure shows a point in time in which the RE is in control.
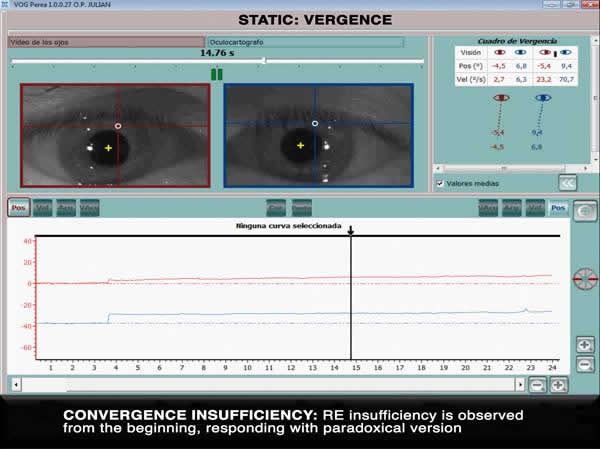
Fig. 10: In this other case,
maintained convergence insufficiency is expressed in the RE from the beginning.
DISCUSSION AND CONCLUSIONS
The authors aim at establishing that examining convergence by means of a guided movement in which the patient looks at an object and if the eyes converge when it is is brought closer the examiner defines it as adequate merely on the basis of his visual assessment is an artificial and incomplete examination procedure because humans never converge their eyes in that manner. The same can be said about the use of prismatic vergences. In both procedures it is not possible to analyze the saccadic-vergence association or to assess sustained vergence.
Static vergences explore an initial and final state. However, the study of dynamic vergences with video-oculography assesses what occurs throughout the movememt at 40 milisecond intervals.
Video-oculography has just begun. The dynamic results discussed above are only the beginning of a research process that, at this date, has no foreseeable limits. When we become able to analyze vergence pathologies associating them with variations of:
1. Latency. The time that elapses between the reception of the order to begin a movement and its actual beginning. In physiology, this value has been estimated between 100 ms and 400 ms, with a mean of 250 ms. these values are similar in convergence and in divergence.
2. Amplitude. The angle formed by the visual axis of each eye in fixed gaze from 1.00 m to 0.15 m. The monocular value ranges between 6 and 13º, with a mean of 10º. It varies depending on the distance between the eyes and the situation of the near point.
3. Velocity. Referred to the velocity of the fast phase of vergence. The normal values we have obtained ranged from 14 degrees/s to 140 degrees/s. These values are similar in convergence and divergence. The mean values are: in convergence 77degree/s and in divergence 83 degrees/s.
4. Morphology of the curve.
5. Vergence execution time, comprising the time elapsed from its beginning up to its end (when the stability phase begins). The normal values are: 0.16s to 0.50s).
... that will be the time when we will understand more about the ocular motor system and about subjective clinic for which today we have no explanation whatsoever.
REFERENCES
-
Perea J. Fisiopatología del equilibrio oculomotor. Pág. 139. Edición: Brosmac S.L. 2011.
-
Perea J. Estrabismos. Pág. 281. Edición: Artes Gráficas Toledo. 2008.
-
Perea J. Estrabismos. Pág. 340. Edición: Artes Gráficas Toledo. 2008.